Day-case knee and hip replacement: a systematic review and meta-analysis.
French et al.
Bone Joint J. 2024;106-B(12):1385-1392.
Over recent years there’s been a major move towards an increasing percentage of surgical procedures being undertaken on a day-case basis, rather than inpatient.
This paper, which is certainly worth reading, is a systematic review and meta-analysis of the published literature on day-case hip and knee replacement surgery. Its results (as described in the full paper, not just the abstract) show that of the patients reported in the observed study, 74% of patients undergoing total knee replacement surgery were discharged from hospital on the same day as their surgery.
Important points to note about studies describing post-op discharge as ‘Day-case’!
First, a majority of the published literature on day-case joint replacement surgery comes from America. In America, their definition of ‘day case’ is where a patient stays in hospital for less than 24 hours. Importantly, this means that ‘day-case’ surgery can actually include an overnight stay… just as long as the overall period in hospital is < 24 hours.
Next, many American hospitals performing ‘day-case’ surgery actually have a facility attached to them where the patients are ‘discharged’ to. I’ve visited some of these centres myself, and in some of them there is literally just a door that you go through where one side of the building is designated as the surgical centre, with the other being a ‘separate’ (on paper!) rehab centre. Clearly, these centres are quite different from a patient being discharged from a hospital back to their own home!
(Remember, the devil is always in the detail… and the best way to manipulate a narrative is to simply change the meanings and definitions of the words that you use!)
The bad old days
In the past, recommended medical advice for post-operative care after orthopaedic procedures erred very much on the over-protective and over-cautious side. For example, patients undergoing ACL ligament reconstruction in the knee had their leg put into a full-length cast for the first 6 weeks before then getting going: by then, their leg was super stiff and they had extreme muscle wasting, both of which severely prolonged overall recovery times. By comparison, nowadays a patient having an isolated ACL reconstruction is encouraged to fully-weight-bear (with the assistance of crutches initially), without a knee brace, and to get their knee going as quickly as reasonably possible, and the importance of early active physiotherapy input is now well-understood.
There is a definite move now towards rapid / early discharge of knee (and hip) replacement patients. Just a few decades ago, a patient undergoing knee replacement surgery in Germany was obliged to stay in hospital for a full 2 weeks before being ‘allowed’ to leave. Nowadays, however, patients are encouraged to leave hospital as quickly as possible.
What are the advantages of getting out of hospital quickly?
There is a long list of potential positives for early discharge from hospital, and these include:
- It’s difficult to rest properly when you’re in a strange environment, not in your own bed, where you’re constantly being interrupted or even woken up by people coming into your room to check on you.
- In many hospitals the food can be less than ideal, in which case you might want to get back home back so that you can eat something decent that you actually like.
- In some hospitals, the staff may be less than 100% friendly and/or their communication skills might be somewhat lacking (a P.C. way of putting this!).
- In many NHS hospitals you might be in a ward with other patients, with what can be an awkward and embarrassing lack of privacy.
- Your ward might have a mix of patients, meaning that there could be people on there with infections of various kinds, which then increases the risk of an infection potentially being passed on to you, which could end up being a disaster!
Importantly, however, if you are in a private hospital with:
- your own private room,
- friendly and attentive nurses, with good communication skills and a happy disposition (because they actually enjoy their jobs!),
- good food,
- low infection rates,
- twice-daily inpatient physiotherapy sessions,
- the full list of whatever painkillers and other drugs that you might need,
- the full range of specialist medical back-up, should (God forbid) you actually end up needing it, and
- as much general help and assistance as you could ever need…
… then why would you ever want to go home prematurely?
I normally operate on my patients at London Bridge Hospital on a Tuesday morning. Most of my knee replacement patients tend to leave hospital on the Friday morning, which is a 3-night stay.
More often than not, when I speak to my patients later on, on the day of their surgery (to let them know how everything went and to reassure them), they’re often groggy from A) the anaesthetic drugs, B) the painkillers and C) from the fact that quite often, people tend not to get a very good night’s sleep the night before they are due for a major operation.
On Day 1 post-op (the Wednesday), a majority of my patients look quite happy and fairly sprightly.
On Day 2 post-op (the Thursday), it’s not uncommon for the patient to have a slump, and for them to look wiped out and a bit miserable! (I normally warn my patients in advance that this might happen.)
By Day 3 post-op (the Friday), the large majority of my patients are happy and ready for discharge. To be deemed ready to home requires input from A) me, the consultant, but, perhaps more importantly, B) the ward nurses, C) the inpatient physios and, of course, D) the patient themselves.
After discharge from hospital, some of my patients (mainly those who are elderly and more frail, and/or those who live alone) then end up going to a rehab centre such as The Clavadel Rehab Centre, in Guildford, for a week or so. At The Clavadel, there is 24-hour nursing care, there are on-site physiotherapists, with a specialist gym and with exceptional hydrotherapy facilities, the environment is specifically geared up towards early post-op rehab, the food is good, the staff are excellent and the level of care provided to patients is 5-star! Centres such as The Clavadel offer a fantastic option to those patients who need a bit of extra support after their surgery.
In whose best interests is it to discharge a patient from hospital early?
A few years ago, a hospital manager asked to have a chat with me. He advised me that my average discharge time was 3.1 days, and he asked whether I could help get that down to < 3. When I asked him why, he simply said that it was ‘for the insurance companies’!!?! My reply back to him was short, curt and to the point!! (Polite, of course, but direct!)
My patients go home when they’re ready, simple as that!
I can’t help but feel that the recent push towards day-case knee or hip replacement surgery is perhaps at best misguided, or perhaps, if one were to take a more cynical view, even somewhat nefarious, as instead of putting the patient’s best interests first, it certain feels as if this agenda is being driven perhaps by:
- hospitals, who are desperate for the beds,
- insurance companies, whose prime focus is reducing costs and thereby increasing profits, and
- some doctors, who come across as being possibly more ego-driven, or even perhaps desperate to create and publicise some kind of ‘USP’ for marketing purposes, rather than this trend necessarily being specifically for the individual patient’s best interests.
Recently, I was at a knee meeting where a team presented their protocols for day-case / 1-night stay knee replacement surgery. In their presentation they stated:
“It’s important to get the patient out of hospital on Day 1 post-op, because by Day 2 and Day 3 they often look a lot worse, and then you’ll never get them out early” (or words very close to that effect).
For me, this says it all… get the patients out whilst they’re still drugged up enough to have that false sense of security in the initial early post-op period, before everything starts to wear off and before they then feel really bad!!?! …. but it’s then, on Day 2 or 3, when the patient is feeling really bad that the patient actually ends up really needing the level of support and care that a decent hospital can actually provide.
I’ve heard horror stories recently, of patients being discharged from hospital early, with absolutely minimal back-up. For example, a patient having a knee replacement being discharged the following day with nothing stronger than just Paracetamol to take home, and a mastectomy patient being discharged on the day of her actual surgery with no spare dressings, and with her being expected to deal with her drain herself, with no real guidance. This is just barbaric, and sounds like Third World medicine! Similarly, I regularly hear of patients being discharged after knee replacement surgery in the NHS with no outpatient physiotherapy having been arranged, and with the patient simply having been given some exercise advice on a few stapled sheets of A4 with line diagrams!
Are there any positives?
Well yes, there are!…
What the drive towards early discharge has done is that is has created significant focus on how best to improve the early post-op care of our patients. So, by adopting many of these tips and tricks, we can actually significantly enhance the comfort levels and overall care of our patients in the initial post-op period, and, importantly, once a patient is on a positive trajectory with their overall recovery, then generally, they tend to continue on that positive upward slope, and they tend to end up with better long-term outcomes.
Some of the key things that we normally include for most of our knee replacement patients in my practice are:
- Pre-hab: it’s important to see a good physiotherapist ahead of knee replacement surgery (rather than just afterwards), as the fitter and stronger you can get yourself ahead of your surgery, then the better you’ll be able to cope with the operation and with the post-op rehab afterwards, and hence the better your overall recovery and your final outcome are likely to be.
- Nerve blocks: our anaesthetist performs an ultrasound-guided subsartorial femoral nerve block whilst the patient is asleep in the anaesthetic room, just before the patient comes into theatre. This numbs the sensory nerves around the knee without affecting the motor nerves to the muscles.
- High-volume peri-capsular Marcaine injection: during the operation I inject local anaesthetic into the back of the knee and around the whole of the joint, which helps reduce early post-op pain.
- Vivostat PRF autologous fibrin sealant: next, towards the end of the operation I spray the cut bone and tissue edges with Vivostat PRF. With this, we take 120ml of blood from the patient’s arm whilst they are in the anaesthetic room: this is then spun down, so that 30 minutes later we have 5ml of PRF, which is ‘platelet-rich fibrin’. PRF is like the sticky part of a blood clot (it is not PRP (platelet-rich plasma), which is pointless!). The PRF acts as a haemostat and it reduces bleeding into the knee: this reduces post-op pain and swelling, which itself aids with early post-op recovery. (READ MORE)
- The Game Ready machine: I am definitely not a fan of the term ‘mandatory’!! However… personally, I think that every patient undergoing knee replacement surgery should use a Game Ready machine (or similar). This is a cuff (attached to a box) that ices the knee whilst applying intermittent pneumatic compression, and it reduces post-op pain and swelling, meaning that patients end up needing less painkillers, and meaning that they can push themselves harder with their early post-op rehab, which then normally improves long-term outcomes.
- Early, regular, intensive post-op physio: one really cannot over-estimate just how important it is that knee replacement patients receive sufficient physiotherapy support post-operatively. My patients normally see the in-patient physios x 2 a day whilst they are in hospital. If my patient has their op on a Tuesday and if they end up going home on the Friday, then I advise them to start their outpatient physiotherapy sessions on the Monday or the Tuesday of the following week: i.e. ASAP! – with just a couple of days of downtime beforehand, over the weekend, to acclimatise to being back home. Ideally, patients should then be seen x 2 (or sometimes even x 3) a week by their local physio, for several weeks, with the frequency of sessions just gradually being reduced as the patient makes sufficient progress (but with the patient still continuing with their exercises themselves, at home, several times a day, every day!
- Back-up: every one of my knee replacement patients has my contact details (including my personal direct email address), the contact details of our practice and the contact details of the orthopaedic ward at the hospital (which is open 24 hours a day, 7 days a week), so that if they do have any queries or concerns, then they are able to get advice rapidly (and pretty much straight way, for anything that might potentially be urgent).
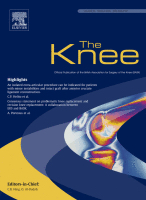
- Custom-made knees: and finally… if you want the very best outcome then you also need the very best prosthesis, and there’s no better knee on the market than a Conformis iTotal patient-specific customised knee prosthesis – the only prosthesis that is guarateed to fit each individual patient’s knee’s size, shape and contours every single time! READ MORE
If all of the above is put in place, then hopefully each and every patient will do well and will achieve a good and happy outcome. This is my aim and my focus, not ‘early discharge’. If a patient does well and if they feel ready and if they want to go home earlier than average, and if that is deemed safe and appropriate, then that’s absolutely fine by me! However, do I, personally, think that day-case or 1-night stay knee replacement surgery is a good thing?… HELL NO!!