
The importance of imaging
When it comes to getting a proper diagnosis, it’s impossible to know exactly what’s going on inside a knee just from looking at the outside (i.e. by just looking at the skin!) – and to truly see what’s really inside a knee one actually needs proper imaging. The imaging options available to us include:
- X-rays
- Ultrasound
- MRI
- CT
- Bone-SPECT scans
Good old-fashioned X-rays
Good old-fashioned X-rays give a lot of useful information, and if a knee joint has fully-blown arthritis, then this might be all that’s needed. It is, however, important to get a full set of appropriate views.

Weight-bearing AP (anteroposterior) view of a knee with medial compartmental arthritis – showing loss of the joint space (due to loss of the cartilage) and bone-on-bone contact.

Lateral knee X-ray
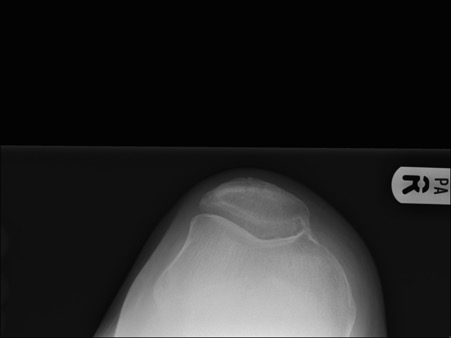
Patellar skyline view
Long-leg weight-bearing alignment X-rays
If there is significant deformity (angulation) present, then it’s also important to get long-leg weight-bearing X-rays too:

Complex deformity, with previous hip problems + shortening of left leg + angulatory deformity + rotational deformity.

Different patient, with valgus angulatory deformity due to severe lateral compartmental osteoarthritis in the right knee.

Same patient, with correction of alignment after appropriate knee replacement surgery.
MRI scans
In mildly arthritic knees, or in cases where you’re not entirely sure exactly what might be going on, or if you want to see whether an arthritic knee might potentially be suitable for a partial replacement instead of a total, then it’s very important to get as much additional information as possible, and this normally requires an MRI scan. MRI shows the bones, the ligaments, the meniscal cartilages, the articular cartilage and much much more – and it’s completely non-invasive and zero risk. The only reason that some people might be against patients having MRI scans is if they’re trying to save money (which is not something that’s in the best interests of the patient) or if they don’t really understand ‘knees’ and they’re not able to put the information that’s gleaned from imaging into appropriate context, by proper interpretation.

MRI scanner.
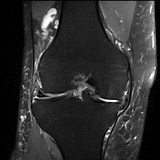
MRI scan showing medial osteoarthritis, but with a seemingly good lateral compartment.
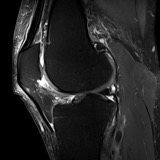
Side view confirms cartilage loss on the back of the patella as well.
CT scanning
When there is metalwork in place within the knee, or if there is bone loss, and/or if there is deformity in or around the knee joint, then CT scanning (which specifically shows the bone in a lot more detail) can be extremely useful:

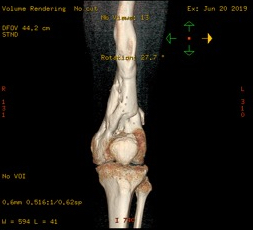
CT of knee showing presence of previous metal screws in the femur from previous surgery.
CT showing complex deformity of distal femur after previous severe femoral fracture in past.
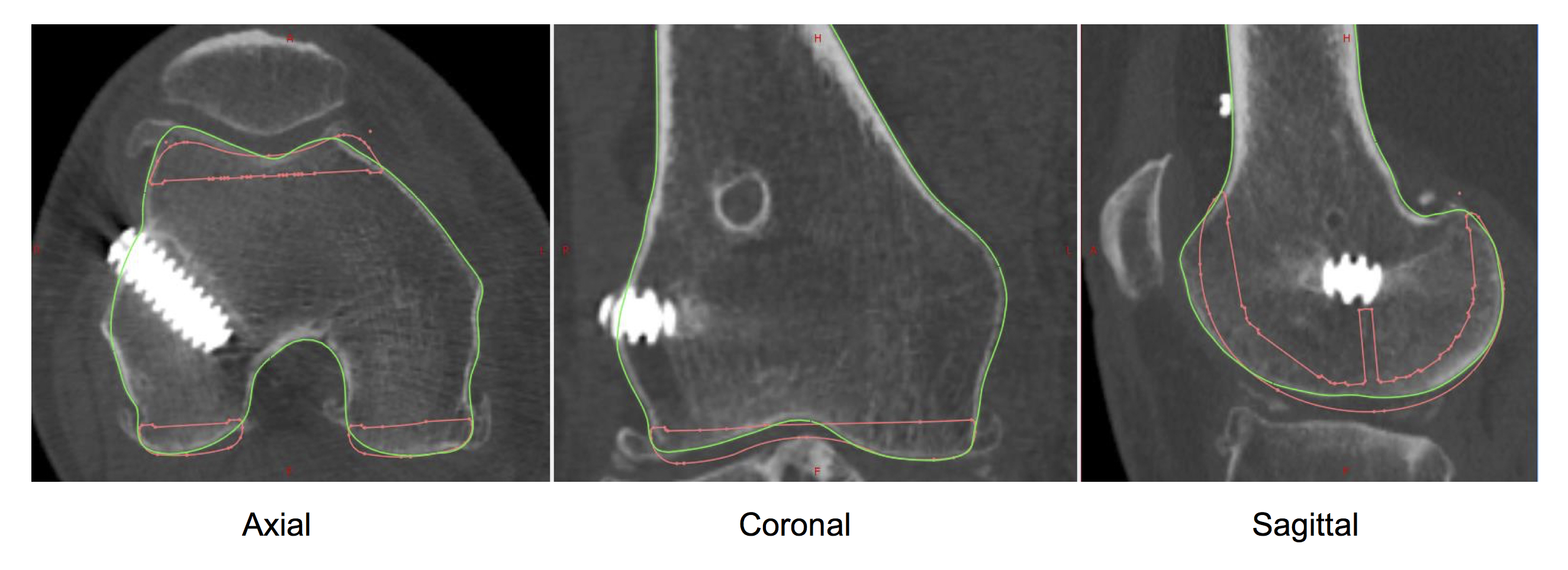
Planning CT for custom-made knee replacement – checking whether previous metalwork will be in the way of the femoral prosthesis.
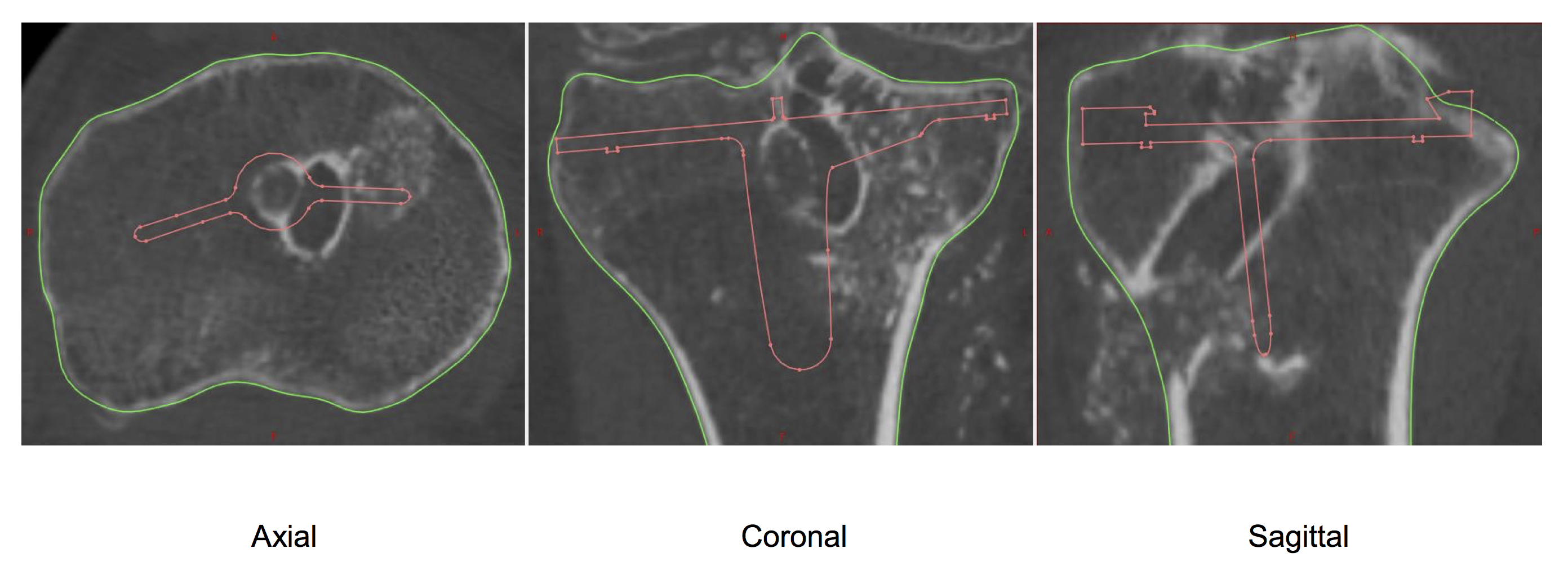
Same patient, with planning views of the proximal tibia, showing tunnels from previous ACL surgery, with bone loss vs position of planned tibial prothesis.
Bone-SPECT scans
Occasionally, even more specialised imaging might be required for some patients, to help diagnosis exactly what the specific location of any pathology around the knee might be. For this, one of the most sensitive and accurate tools is a SPECT scan – Single-Photon Emission Computerised tomography – which shows any potential ‘hot spots’ of increased metabolic activity in the bone within a very precise anatomical location:
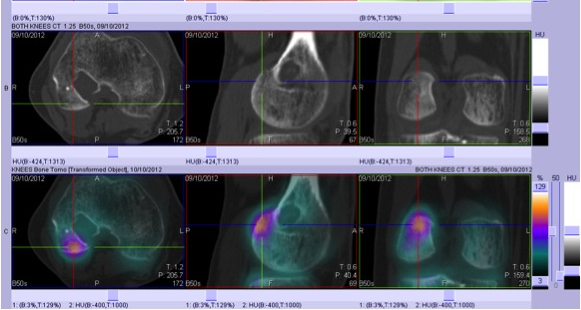
Images from a SPECT scan showing a ‘hot spot’ at the back of the lateral femoral condyle.
What to do?
So, if you want to know:
- what’s actually wrong with your knee, and
- what your full range of options might be,
then
- go and see a Consultant Knee Surgeon,
- have a full and detailed history taken, and have a proper clinical examination,
- have the full set of whatever potential imaging might be required for your knee, and then
- have a proper discussion with your knee specialist about your knee.
Don’t allow anyone to talk to you about treatments until you’ve first got an actual Diagnosis – and this nearly always requires imaging!
Written by:
Mr Ian McDermott
Consultant Knee Surgeon, London
13th April 2020